Can the Thickness of the Aorta Be Determined Before Heart Surgery?
Facts and Misconceptions**
When heart surgery is mentioned, many people ask the same question: ‘Can doctors determine how strong the main artery coming out of the heart – the aorta – is before surgery?’
This curiosity is quite natural. However, there are some misconceptions circulating about this topic. Let’s explain this important issue in a way that everyone can easily understand.
Why is the Aorta Such a Vital Artery?
The aorta is the largest artery that carries blood from the heart to the entire body. Blood going to the brain, reaching the kidneys, and flowing down to the legs all passes through this artery.
During heart surgery:
- The aorta is touched,
- Sometimes the aorta is opened,
- Sometimes the connection to the heart-lung machine is made through this artery.
Therefore, a weak aorta poses a serious risk during surgery.
Misconception: ‘CT Scans Show the Aortic Wall’
A commonly heard statement in society is:
‘I had a contrast-enhanced CT scan, and they said the artery is fine.’
However, the reality is different.
CT scan:
- It can show the width of the vessel,
- The blood flow inside it,
- Large tears or bulges.
But it is not possible to see whether the aorta wall is actually thin, thick, or strong with a CT scan. This is a condition that cannot be clearly measured even with today’s medical capabilities.
So what do doctors do before surgery?
Surgeons look at certain indicators before surgery:
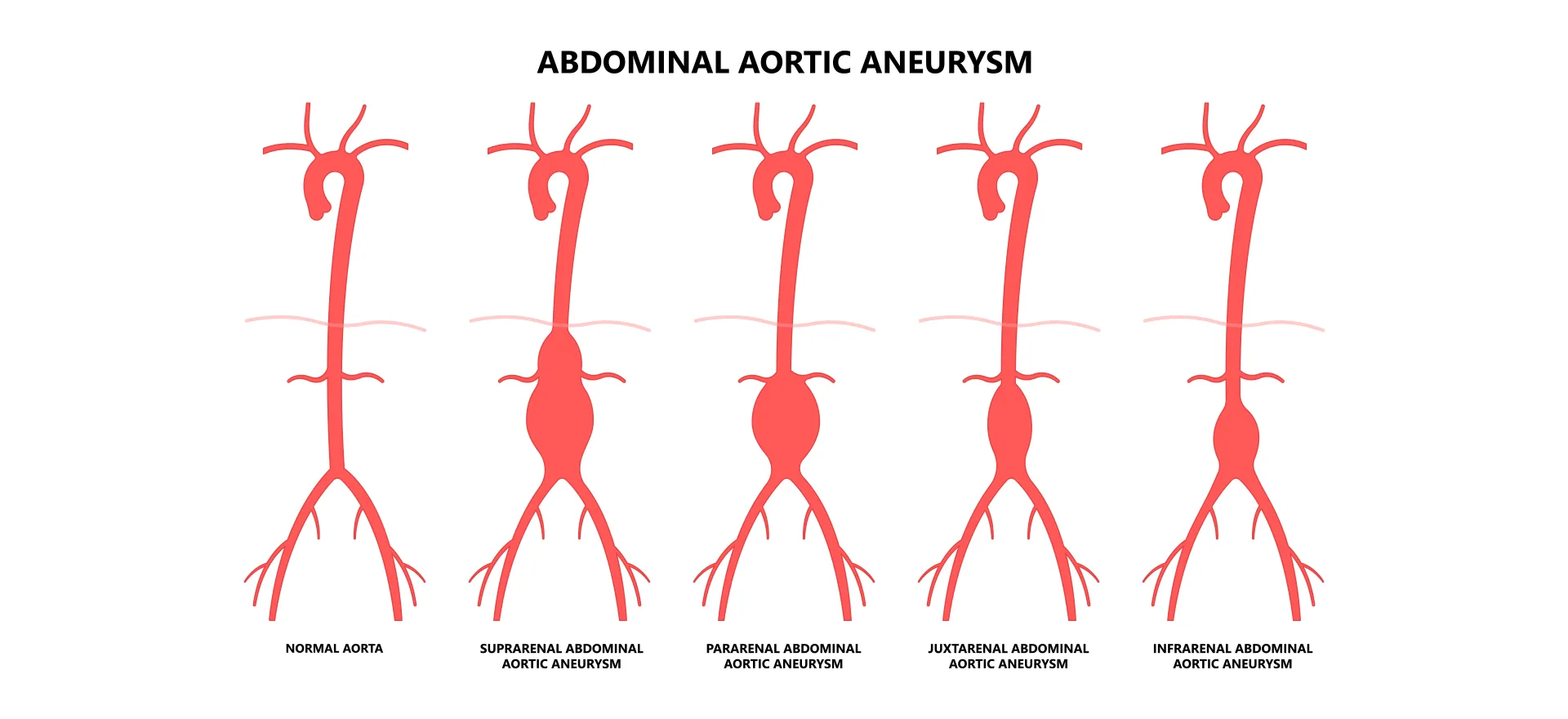
- Is the aorta wider than normal?
- Has the patient had high blood pressure for a long time?
- Is there calcification in the artery wall?
- Has the patient had heart surgery before?
These findings provide clues that the artery may be weak. But they are not definitive.
Therefore, doctors:
- Do not say, ‘This artery is definitely thin,’
- But rather, ‘There may be a risk with this artery,’ and plan the surgery more carefully.Another Misconception: ‘The Surgeon Can Tell Just by Looking’
Some people think:
‘The surgeon can tell if the artery is thick or thin just by touching it with their finger during surgery.’
This is also incorrect.
A vessel:
- May feel hard externally but have a very thin wall,
- May appear normal externally but have a thin and weak wall.
Touching it only reveals its hardness; not the thickness of its wall.
These two concepts should not be confused.
When Does the Truth Emerge?
The true condition of the aorta is only understood during surgery, when the vessel is opened.
- When the vessel is cut,
- When the inner and outer layers are visible,
- When the behaviour of the tissue is observed while suturing,
the surgeon obtains definitive information about the vessel’s integrity.
This is the most reliable assessment method in medicine.
What Does This Mean for Patients?
This reality means:
- Doctors do not conceal anything.
- However, some information may not be known with certainty before surgery.
- Therefore, surgeons always enter surgery prepared.
- If necessary, the plan can be changed during surgery. They enter surgery with a Plan B in case of vessel rupture.
The goal is always the same: to bring the patient out of surgery as safely as possible. Changing the surgical plan is also aimed at safely bringing the patient out of surgery.
During heart surgery, aortic rupture (aortic dissection) is a very rare but possible occurrence that changes the entire framework and plan of the surgery. It increases the risk of surgery and is a life-threatening situation. The procedure involves replacing the torn section of the aorta with an artificial vessel. This may sound simple, but the difficulty and uncertainty of the outcome can only be understood by surgeons specialising in cardiac surgery. Having worked at Siyami Ersek Hospital for many years and performed thousands of cases, I have witnessed such situations occur to myself and many of my fellow cardiac surgeons. The development of aortic dissection during heart surgery is unpredictable. This is because there is currently no test that can detect the thickness or weakness of the aortic wall before surgery. Only intravenous ultrasound (ultrasound performed by inserting a probe into a vein) can provide information. However, considering that examining all vessels using this method would take dozens of hours and can only be performed in an angiography laboratory, the routine use of intravenous ultrasound as a preoperative preparation test is not feasible either in our country or worldwide.
Conclusion: Not Something to Fear, but a Reality That Needs to be Properly Understood
- The true strength of the aorta cannot be accurately measured before surgery.
- Imaging tests only serve to estimate risk.
- Looking or touching from the outside is not sufficient.
- The most accurate assessment is made when the vessel is opened.
For this reason, heart surgeries are performed by experienced teams with backup plans.
This uncertainty is not a shortcoming; it is a natural part of the conscious, controlled, and safe approach of modern cardiac surgery.